


Knee pain is an extremely common finding and it can affect individuals of all ages. Not all knee injuries are equal and fortunately not all knee injuries are serious. The art is to find which are serious and which are not!
Pain is an interesting phenomenon. It’s simply just a signal our brains send to tell us to be aware of the area that has either sustained an injury or is vulnerable to sustain an injury. But there are cases where pain is simply a misfire (yes our brain can mess up too) and so there’s a lot of conditions that just kind of go away.
Although there is no accurate way of self diagnosing knee conditions there are some findings that can help us break down how badly the knee is injured and if wait and rest the best option!
What happened?
1) The first part of any diagnosis starts with a history because it can tell us a lot about our conditions. First part is where on the knee does it hurt? (*please note that without a full history it is always challenging to diagnose and the listed are not an exhaustive list but just grouping them based on location)
Let’s use this diagram to break down the areas based on the colors (least severe to most severe).
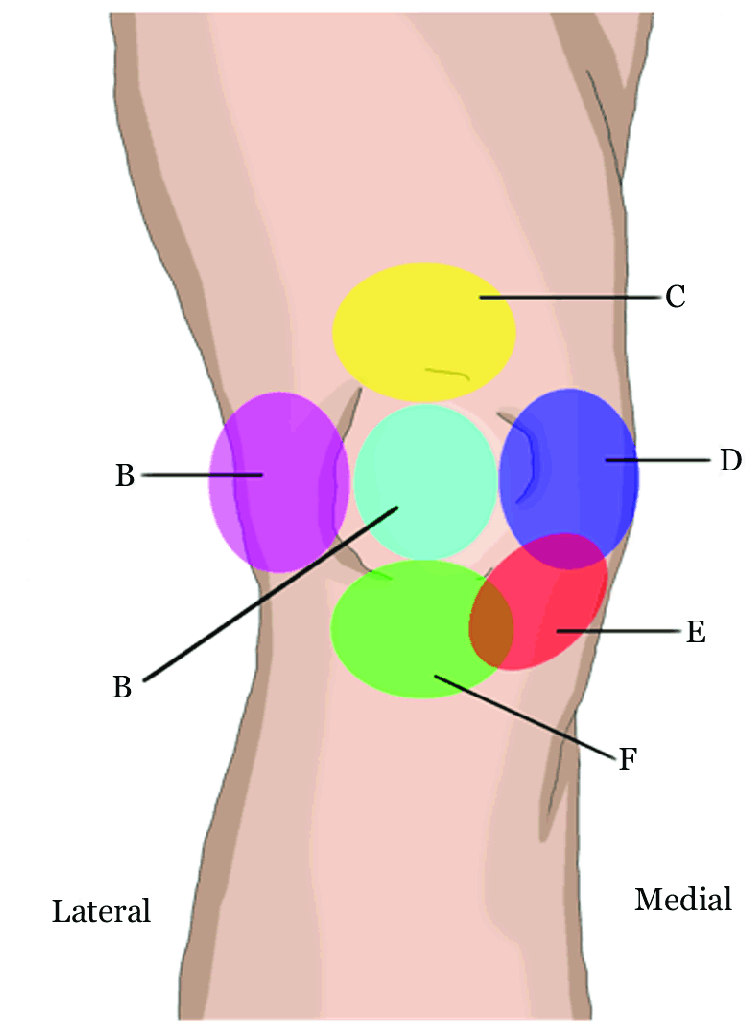
- Magenta (outside of the knee): Iliotibial Band Syndrome (IT band syndrome, Lateral Collateral Ligament (LCL) Sprain, Lateral Meniscus Tear
- Green (below the kneecap): Infrapatellar tendonitis (jumper’s knee), Osgood Schallater’s disease (children condition), Osteochondritis Dessicans (with trauma), Tibial Plateau Fracture (with trauma)
- Cyan (Knee cap): Patellofemoral Pain Syndrome, Chondromalacia Patellae, Arthritis (gradual onset), Patellar fracture
- Yellow (above the knee cap): Suprapatellar tendonitis (tight quads)
- Dark Blue (inside of the knee): Adductor muscle strains, Medial Collateral Ligament (MCL) sprain , Medial Meniscus Tear, Arthritis
- Red (lower inside corner of knee): Pes anserine bursitis, Medial Plica Syndrome
2) How did it start?
- Was it traumatic, was it gradual? A lot of the conditions listed are different based on what created the condition. In the knee, the more serious conditions are usually due to trauma or impact activities and the less serious conditions are usual gradual onset and typically a repetitive stress injury ie: patellofemoral pain syndrome, IT band syndrome, Pes anserine bursitis, Medial Plica Syndrome, Jumper’s knee and suprapatellar tendonitis. Whereas the more traumatic conditions typically can cause the MCL, LCL, Meniscus, various fractures and even the ACL (anterior cruciate ligament) which was not described by location.
3) Is it getting worse, better or staying the same?
- This question is to check to see if the condition has changed since it started. Of course worsening means you likely need to get it assessed whereas getting better has a higher likelihood of recovering on its own
4) What is the quality of the pain?
- Is the pain sharp? Is it dull? Does the knee feel unstable? Are you able to put weight on it?
- ***If any of the instability or inability to place weight on the leg occurs then you should go seek help as those are never good signs for the knee.
5) How bad does it hurt?
- Is it just simply a 1-4/10 pain where it is minor and noticeable or is it 7-10/10 where it is unbearable? The unbearable pain levels will signify a need to get checked out
6) Is it swollen, did it bruise, are you able to bend it?
- If there is massive swelling that prevents motion, significant bruising or just any challenges of loading or moving then it warrants getting assessed. One of the screens for a broken bone is can we walk four steps? If that is impossible then it is time to get it assessed.
Who should I go to in order to assess my knee?
This is a very loaded question as many professionals can help you. Let’s break it down into severity.
- If you are unable to walk and load that leg, you will likely need some type of imaging in order to rule out broken bones and possibly any torn ligaments. Typically, an x-ray will be the first imaging and it can only show if any broken bones have occurred. If nothing is found it does not mean nothing is damaged. The next step that may occur is further imaging such as diagnostic ultrasound, CT scan or MRI but often times these take time before you can obtain these tests. So in the meantimes it would be best to get an assessment from a manual practitioner such as a physiotherapist or chiropractor who works on cases outside of the spine. Often times, even torn ligaments can be rehabbed and it is suggested that these solutions should be attempted before any surgical intervention is suggested.
- If you are able to walk, but there is any instability, or severe pains and limitations then it is suggested to see a manual practitioner who can assess you for any of the above conditions. Typically it would be a physiotherapist or a chiropractor that works on cases outside of the spine. After a bunch of orthopedic tests and motion screens, there should be some working diagnoses to help you with the knee condition and get you back to normal.
How do I rehab my knee?
Our philosophy on the knee is that it is like a middle child in the chain between the older child (the hip) and the younger child (the ankle) and as a result, the middle child always screams out first when anything happens. Especially in repetitive stress conditions like ITB syndrome, tendonitis, bursitis, etc. these conditions are based on overuse of tissues. So how we help these conditions are to release the muscle tensions and then retrain the body to load forces into the correct areas. Frequently, our approach to these cases is to loosen the guarding muscles around the knee and then strengthen and stabilize the hip.
Here’s a few examples of loosening muscles
Foam roller on quads
Adductor foam roll
And strengthening the hips:
Hip airplane
Fire Hydrants
Standing Fire Hydrant:
1) Place a resistance band around your knees and stand up.
2) Bend one leg slightly and lift your opposite foot off the floor-bend that knee slightly.
3) Without moving your trunk, rotate the leg toward the outside ( so that you are externally rotating your hip)
4) Return to the starting position. Repeat 10 times.
5) Repeat on opposite leg if necessary.
Quadruped Fire Hydrant:
1) Start on all fours with your back flat.
2) Keeping your knee bent, raise one leg out to the side at a height that allows you to keep your pelvis and shoulders parallel to the floor.
3) Return to the starting position. Repeat 10 times.
4) Repeat on the opposite side.
Banded squats
As always, if you have any questions about your conditions and would like to schedule an appointment with us at Baseline Health and Wellness you can give us a call at 6046744027 or schedule online at www.baselinewellness.ca
Provided by Dr. Kody Au, Vancouver Chiropractor
*Disclaimer*
The information contained in the multimedia content now stated as “Content” posted represents the views and opinions of the original creators of such Content.
The Content has been created and shared for informational and educational purposes only. Baseline and it’s practitioners do not make any warranties or guarantees with respect to the accuracy, applicability, fitness, or completeness of the Content. Baseline does not warrant govern over the effectiveness or applicability of any sites linked or provident in the Content.
The Content is not intended to be a substitute for professional history, exam, diagnosis or treatment. Ensure that you always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Do not disregard professional medical advice or choose to delay in seeking medical care because of something you have read or seen on the Site.
Baseline hereby disclaims any and all liability to any party for any direct, indirect, implied, punitive, special, incidental or other consequential damages arising directly or indirectly from any use of the Content, which is provided as is, and without warranties.